
When you pick up a generic pill at the pharmacy, you might assume it’s just a cheaper version of the brand-name drug. But behind that simple swap is a rigorous scientific process designed to make sure it works just as well. That process is called bioavailability testing - and it’s the backbone of how the FDA approves generic medications. Without it, we wouldn’t know if a generic drug actually does what the original does. So what exactly do these studies test? And why does it matter?
What Bioavailability Really Means
Bioavailability isn’t just about whether a drug gets into your body. It’s about how fast and how much of it gets there - and whether that amount is enough to have the same effect as the brand-name version. The FDA defines it as "the rate and extent to which a therapeutically active chemical is absorbed from a drug product into the systemic circulation and becomes available at the site of action." In plain terms: if your heart medication doesn’t reach your bloodstream at the right time and in the right amount, it won’t work.
Two key numbers measure this: AUC and Cmax. AUC stands for Area Under the Curve - it tells you how much of the drug your body is exposed to over time. Think of it like the total dose you get. Cmax is the highest concentration the drug reaches in your blood. That tells you how quickly it gets absorbed. Together, they give scientists a full picture of how your body handles the medicine.
For example, if a generic drug has an AUC that’s 90% of the brand-name version, it means you’re getting almost the same total exposure. If the Cmax is within 15% of the original, absorption speed is similar. But it’s not enough to just look at averages. That’s where confidence intervals come in.
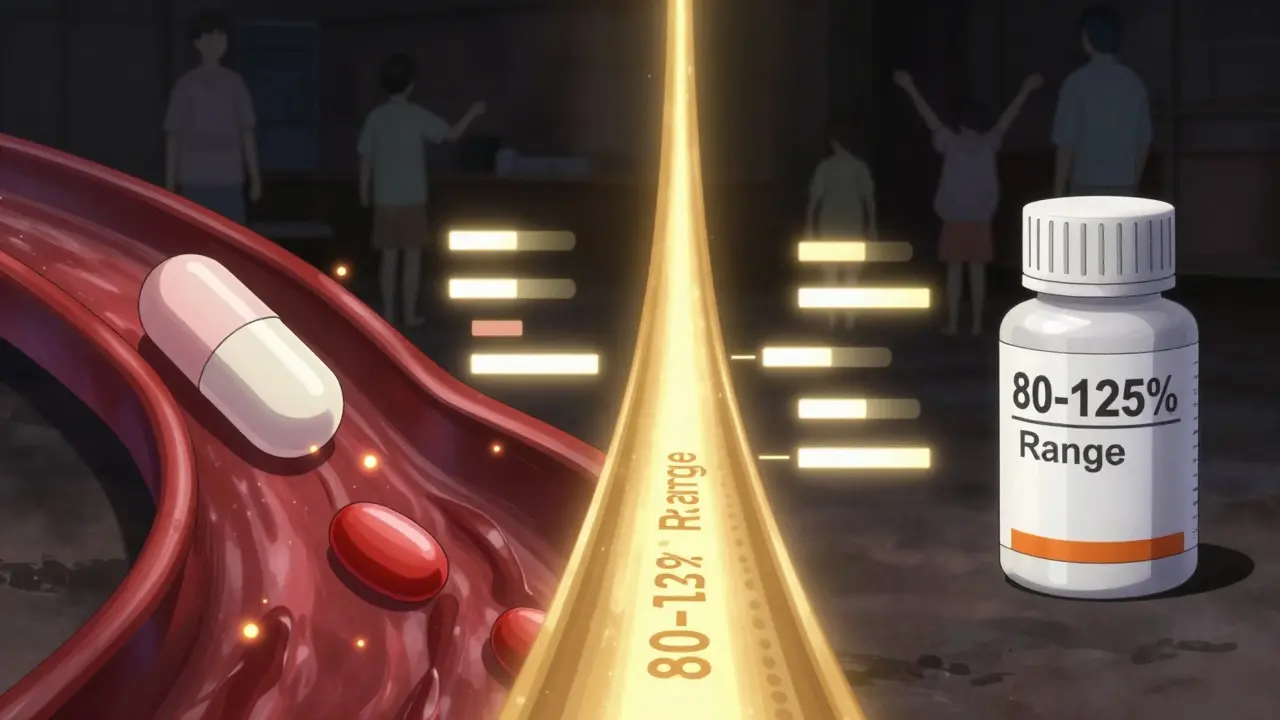
The 80-125% Rule: Why It’s Not Arbitrary
Here’s the rule that every generic must pass: the 90% confidence interval for both AUC and Cmax must fall between 80% and 125% of the brand-name drug. That means the true difference between the two can’t be more than 20% in either direction - and even then, the average difference is usually much smaller.
This range isn’t pulled out of thin air. It’s based on decades of clinical data. Studies show that a 20% difference in absorption rarely affects how well a drug works for most people. For example, if a blood pressure pill’s generic version delivers 15% less drug, your blood pressure still drops just as effectively. But for drugs like warfarin or digoxin - where even small changes can be dangerous - the range tightens to 90-111%.
What’s more, the FDA doesn’t just check if the average is close. They require that the entire range of possible differences (the confidence interval) stays within limits. This means even if the average looks perfect, if one person in the study had an unusually high or low response, the whole batch could fail. It’s a safety net.
How the Studies Are Done
Most bioequivalence studies involve 24 to 36 healthy volunteers. They don’t have the condition the drug treats - they’re used because their bodies respond predictably. Each person takes both the generic and the brand-name version, in random order, with a washout period of at least five half-lives between doses. This ensures no leftover drug from the first dose affects the second.
Blood samples are taken every 15 to 60 minutes for up to 72 hours. For a drug with a 12-hour half-life, you might sample 16 times. The samples are analyzed using highly accurate lab methods that must be validated to within 85-115% accuracy. If the lab’s results are off by even 5%, the whole study is invalid.
For example, one study showed a generic with an AUC ratio of 1.16 - meaning it delivered 16% more drug than the brand. At first glance, that sounds fine. But when the upper limit of the confidence interval hit 1.30, the product failed. Why? Because the FDA can’t rule out that some patients might get 30% more drug - which could cause side effects.
When the Rules Get Tricky
Not all drugs are created equal. Some, like levothyroxine (used for thyroid conditions), are highly sensitive. Small changes in absorption can lead to symptoms like fatigue, weight gain, or heart palpitations. That’s why many doctors still prefer brand-name versions for these drugs - even though the FDA says they’re equivalent.
Then there are extended-release pills, inhalers, and topical gels. These aren’t just swallowed and absorbed. Their design matters. A slow-release tablet that releases drug over 12 hours must match the brand’s release pattern at multiple time points - not just at peak. For inhalers like budesonide, scientists can’t measure blood levels easily. Instead, they use lung deposition tests and clinical outcomes like asthma control.
Highly variable drugs - like tacrolimus or certain antibiotics - are another challenge. Some people absorb them quickly, others slowly. To handle this, the FDA now allows "scaled average bioequivalence," which widens the acceptance range (to 75-133%) if the drug naturally varies a lot in the body. This keeps safe generics on the market without forcing unrealistic standards.
What About Patient Stories?
You might have heard stories: "My seizure came back after switching generics," or "I got dizzy when they changed my pill." These are real. The Epilepsy Foundation tracked 187 such reports between 2020 and 2023. But after investigation, only 12 cases (6.4%) were possibly linked to bioequivalence issues. The rest were due to missed doses, stress, or other factors.
On the flip side, pharmacists who’ve run hundreds of studies say they’ve never seen a generic fail in real-world use after passing the test. One pharmacist with 12 years of experience said: "In 47 studies, every generic that passed BE performed identically in simulated patient populations."
The FDA estimates 90% of people can’t tell the difference between brand and generic. That’s not luck - it’s science. The system works because it’s designed to catch even small risks before the drug hits the market.
What’s Next for Bioequivalence?
The field is evolving. In 2023, the FDA started using artificial intelligence to predict bioequivalence from formulation data. In a trial with 150 drugs, an AI model predicted AUC ratios with 87% accuracy. That could mean fewer clinical trials in the future.
Also, the FDA now allows "BCS waivers" for certain drugs. If a drug is highly soluble and highly absorbable (BCS Class 1), and the generic matches the brand exactly in ingredients and dissolution, the agency may skip human studies entirely. This saves time and money - without sacrificing safety.
But complexity is rising. In 2015, only 8% of generic applications involved complex products. By 2022, that jumped to 22%. That’s why the FDA launched its Complex Generic Products Initiative, releasing 11 new guidances for tricky drugs like testosterone gels and inhaled corticosteroids.
Why This Matters to You
Generics make healthcare affordable. In the U.S., they make up 97% of prescriptions but only cost 26% of what brand-name drugs do. That’s billions saved every year. But none of that would be possible without bioavailability studies.
They’re not just paperwork. They’re the bridge between science and safety. Every time you take a generic pill, you’re benefiting from blood samples taken in labs, statistical models built over decades, and regulators who won’t approve a drug unless they’re certain it’s as good as the original.
So next time you choose a generic, know this: it didn’t just get approved because it’s cheaper. It passed a test that’s stricter than most people realize.
Do all generics need bioavailability studies?
Almost all oral generics do. But some drugs qualify for waivers under the Biopharmaceutics Classification System (BCS). For example, BCS Class 1 drugs - those that are highly soluble and highly absorbable - may skip human studies if the generic matches the brand exactly in ingredients and how it dissolves. This applies to common drugs like atorvastatin or metformin. But for extended-release pills, inhalers, or drugs with narrow therapeutic windows, human studies are always required.
Can a generic fail bioequivalence testing?
Yes. About 5-10% of generic applications fail the first time. Reasons include differences in inactive ingredients, manufacturing processes, or how the drug dissolves in the body. One example: a generic version of a heart medication failed because its tablet dissolved too slowly in the stomach, leading to a Cmax that was 25% lower than the brand. The company had to reformulate and retest. Failed products are not approved - and can’t be sold.
Why do some doctors still prefer brand-name drugs?
For drugs with a narrow therapeutic index - like warfarin, levothyroxine, or certain anti-seizure meds - even small differences in absorption can matter. While the FDA considers generics equivalent, some doctors have seen rare cases where patients had unexpected reactions after switching. Because these drugs require precise dosing, some providers choose to stick with the brand to avoid any risk, even if it’s small. This isn’t about distrust in generics - it’s about minimizing variables in sensitive cases.
Are bioequivalence studies the same worldwide?
For most standard oral drugs, yes. The FDA, European Medicines Agency (EMA), and Japan’s PMDA all use the same 80-125% range and similar study designs. This alignment comes from international guidelines under the ICH. But for complex products - like inhalers, patches, or injectables - each region may have its own specific requirements. For example, the EMA sometimes requires additional clinical endpoints for topical creams, while the FDA may rely more on pharmacokinetic data.
How long does a bioequivalence study take?
A single study usually takes 6 to 12 months from start to finish. That includes recruiting volunteers, conducting the dosing phase (which lasts 1-3 weeks), analyzing blood samples, and writing the report. The FDA review of the full application can add another 10-18 months. But for generics with BCS waivers or those using new AI-based models, the timeline could shrink significantly in the coming years.

Stephen Habegger
March 21, 2026I’ve been taking generics for years and never had an issue. The science here makes sense - if the FDA says it’s equivalent, I trust it. Saves me hundreds a year.
Linda Olsson
March 21, 2026Of course they say it’s equivalent. They’re paid by the pharma lobby. Have you ever seen the raw data? No? Then you’re just repeating propaganda.
Lauren Volpi
March 21, 2026So what you're saying is, we're trusting a government agency that can't even keep the lights on in a post office to decide if my heart med won't kill me? Yeah right.
Melissa Stansbury
March 21, 2026I switched generics last year and my anxiety spiked. Coincidence? Maybe. But I’m not taking the risk again. My body knows.
cara s
March 23, 2026The statistical rigor underpinning bioequivalence protocols is, in fact, a triumph of regulatory science. The confidence interval methodology, grounded in frequentist inference, ensures that population-level variability is accounted for with a margin of error that is both clinically and statistically defensible. One must appreciate the elegance of this design.
Amadi Kenneth
March 23, 2026They say 90% can’t tell the difference... but what about the 10%? Who’s paying for their ER visits? Who’s covering the lawsuits? This isn’t science - it’s cost-cutting with human lives as collateral.
Shameer Ahammad
March 25, 2026The notion that 'generic equals equivalent' is a fallacy perpetuated by corporate interests. Bioavailability is not a binary variable - it is a spectrum, and the 80-125% range is a grotesque oversimplification of human pharmacokinetics. One must question the ethics of such a threshold.
Alexander Pitt
March 26, 2026The AI models are promising. They’ve been validated against real-world PK data and can reduce trial costs by up to 40%. It’s not about cutting corners - it’s about being smarter. The FDA isn’t lazy, they’re adaptive.
Manish Singh
March 28, 2026In India, we’ve been making generics for decades - and exporting them globally. The quality control is stricter than most people think. If it passes FDA standards, it’s safe. Trust the process, not the fear.
Nilesh Khedekar
March 30, 2026I read somewhere that 1 in 5 generics have different fillers... like talc or cornstarch. What if you’re allergic? No one tells you that. And the FDA doesn’t test for allergies. Just... hmmm.
Robin Hall
March 30, 2026The 80-125% rule was established in 1981. Since then, we’ve had 300,000+ deaths from adverse drug reactions. Coincidence? Or systemic failure? The math doesn’t lie - the system does.
jared baker
March 30, 2026Simple truth: if your drug works fine on brand, stick with it. If it’s cheaper and works just as well? Great. But don’t let anyone scare you - the system’s not perfect, but it’s way better than nothing.
Michelle Jackson
April 1, 2026I switched to a generic for my thyroid med and gained 20 lbs. My doctor said 'it's the same'. No it's not. My body said otherwise. Why do they ignore real people?
David Robinson
April 1, 2026You think this is about science? It’s about profit. Brand-name companies make billions. Generics cost pennies. The FDA’s ‘rigorous’ testing? A show. The real test is whether the stock price goes up.
Andrew Mamone
April 2, 2026This is why I love science. 🔬 The fact that we can quantify absorption, model confidence intervals, and refine standards over decades? That’s progress. Not perfect, but damn impressive. Generics saved my family $12k last year. I’m grateful.