If you're dealing with an overactive bladder, these drugs can feel like a miracle at first. But for a specific group of people-especially men over 65-the risk of a total bladder shutdown is real. In fact, clinical reviews suggest that while only 0.5% of the general population faces drug-induced retention, that number jumps to about 4.3% for men with enlarged prostates. It's not just a mild side effect; it's a significant clinical risk that can lead to emergency room visits and catheterization.
How Anticholinergics Stop Your Bladder
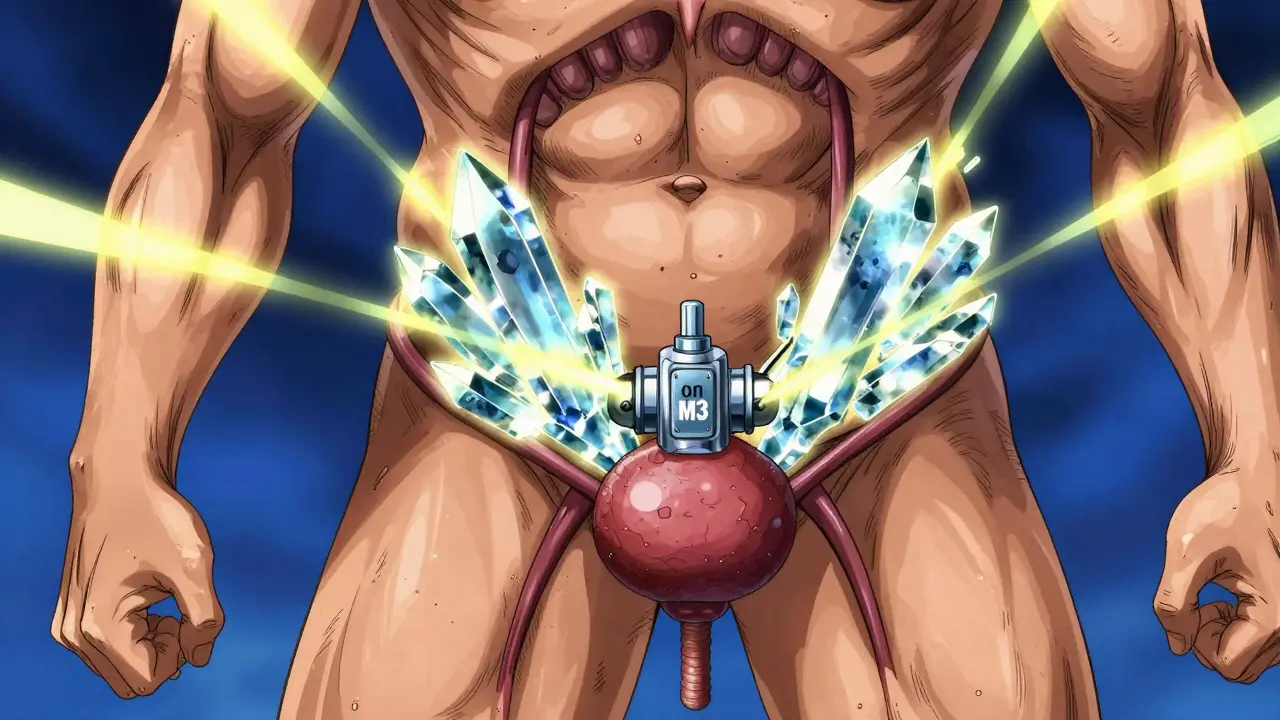
To understand why these drugs cause trouble, you have to look at how the bladder actually works. Your bladder is essentially a muscular bag. To empty it, your body uses a neurotransmitter called acetylcholine, which binds to M3 receptors is the specific muscarinic receptors responsible for triggering the detrusor muscle to contract and push urine out . Think of the M3 receptor as the "on switch" for peeing.
Anticholinergic medications work by blocking that switch. By preventing acetylcholine from binding to the M3 receptors, the bladder muscle stays relaxed. This is great for stopping accidental leaks, but if the block is too strong or the patient already has a narrow exit (like a swollen prostate), the bladder simply cannot contract enough to overcome the resistance. You end up with a "lazy" bladder that holds onto urine long after it should have let it go.
The Risk Hierarchy: Not All Drugs Are Equal
Not every drug in this class carries the same level of danger. Some are "non-selective," meaning they hit multiple receptors throughout the body, while others are more targeted. For example, Oxybutynin is a non-selective anticholinergic drug approved in 1975, known for high efficacy but a higher risk of urinary retention . Because it doesn't discriminate between receptor types, it often carries a higher risk profile. In men with benign prostatic hyperplasia (BPH), the odds of experiencing retention are significantly higher with oxybutynin than with more selective options.
On the other hand, newer drugs like Solifenacin are designed to be more selective for M3 receptors, which can sometimes result in a more predictable response, though the risk is still present. Doctors often use the Anticholinergic Cognitive Burden (ACB) scale to track how many of these drugs a patient is taking. If your total score hits 3 or higher, your risk of urinary retention can spike by as much as 68%, especially if you're an older adult.
| Medication | Selectivity | Risk Level | Typical Incidence |
|---|---|---|---|
| Oxybutynin | Non-selective | High | 1.8% - 2.5% |
| Trospium Chloride | M1/M3 Affinity | Moderate-High | 1.5% - 2.2% |
| Solifenacin | M3 Selective | Moderate | 1.2% - 1.8% |
| Mirabegron (Beta-3 Agonist) | B3 Receptor | Very Low | ~0.3% |
Who is Most at Risk?
The danger isn't the same for everyone. The biggest red flag is Benign Prostatic Hyperplasia (BPH), a non-cancerous enlargement of the prostate gland that compresses the urethra . When the prostate is enlarged, the bladder already has to work overtime to push urine through a narrow straw. If you then add a medication that weakens the bladder's contraction, the system can fail entirely.
Age is another massive factor. The 2019 Beers Criteria-a guide for safe medication use in seniors-lists anticholinergics as potentially inappropriate for older adults. This is because aging organs don't process these drugs as efficiently, and the risk of combined side effects (like confusion and retention) is too high. Polypharmacy, or taking multiple medications at once, further compounds this. For instance, combining anticholinergics with opioids can increase the risk of retention to nearly 13% in some elderly populations.
Safer Alternatives and Better Management
Because the risks are so high, many urologists are moving away from these drugs for men. A popular alternative is Mirabegron, a beta-3 adrenergic agonist that relaxes the bladder muscle without blocking acetylcholine . Instead of stopping the "on switch," it helps the bladder hold more urine by stimulating different receptors. The results are stark: the risk of retention with mirabegron is a tiny fraction of what you see with anticholinergics.
If a doctor does decide to use an anticholinergic, they shouldn't just "prescribe and forget." Proper management involves a few key steps:
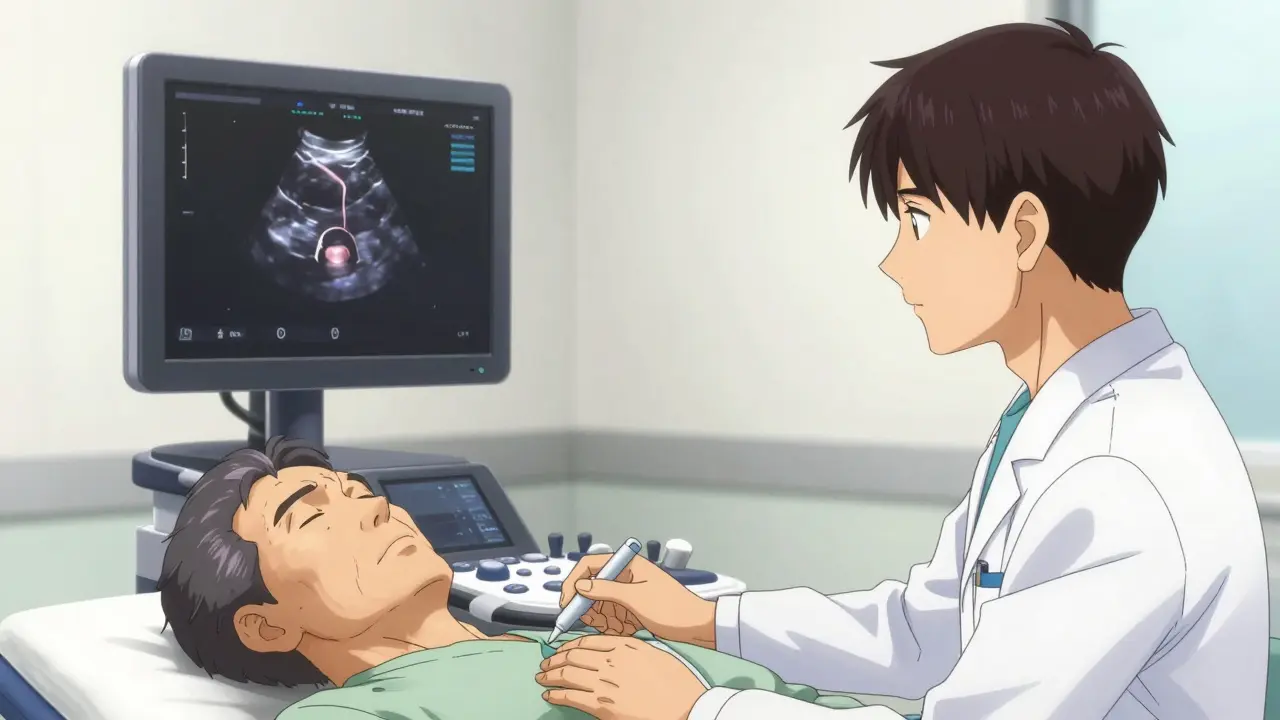
- Baseline PVR Measurement: Before starting the drug, you need a Post-Void Residual (PVR) test. This uses an ultrasound to see how much urine is left in your bladder after you pee. If you already have more than 150mL left over, these drugs are usually a no-go.
- Slow Titration: Starting with a very low dose (around 25% of the standard amount) and increasing it slowly over two weeks can help the body adapt.
- Using Alpha-Blockers: Taking an alpha-blocker alongside the treatment can help open up the prostate area, potentially reducing the risk of retention by over 30%.
- Transdermal Patches: Using a skin patch instead of a pill can sometimes lower the risk of acute retention.
Recognizing the Warning Signs
You shouldn't wait for a total blockage to seek help. There are subtle signals that your bladder is struggling to keep up. Keep an eye out for the "danger signs": straining more than usual to start peeing, a stream that has become noticeably weaker, or a persistent feeling that your bladder isn't actually empty after you've finished.
If you find yourself unable to urinate for 12 hours, or if you experience sudden lower abdominal pain and swelling, head to the emergency room immediately. Acute retention can lead to kidney damage if the urine backs up into the renal system. It's a frightening experience, but it is treatable through immediate catheterization to drain the bladder.
Are anticholinergics safe for women?
Generally, yes. They remain a first-line treatment for women with overactive bladder because women don't have a prostate that can block the urinary exit. While retention can still happen, the incidence is significantly lower (around 5.1% compared to 12.3% in men).
What is a "Post-Void Residual" (PVR) test?
A PVR test measures the amount of urine remaining in the bladder immediately after you void. It is usually done via a quick, non-invasive bladder scan (ultrasound). A residual volume over 150mL is typically a signal to avoid anticholinergic drugs.
Can I stop taking these meds suddenly if I notice issues?
You should always consult your doctor before changing your dosage, but if you cannot urinate at all, this is a medical emergency. Seek immediate care. If you only notice a weakening stream, call your urologist to schedule a PVR check.
Why are beta-3 agonists considered safer?
Unlike anticholinergics, which block the muscle contraction needed to pee, beta-3 agonists like mirabegron work by relaxing the bladder during the filling phase. They don't interfere with the "emptying" mechanism, which is why the risk of total retention is so much lower.
Does age really matter that much for this risk?
Yes. Older adults often have a combination of reduced muscle tone in the bladder, potential prostate enlargement, and other medications (polypharmacy). This "perfect storm" makes them much more susceptible to drug-induced urinary retention.
Next Steps for Patients and Caregivers
If you or a loved one are currently taking an anticholinergic, don't panic, but do be proactive. Start by reviewing all current medications with a healthcare provider to calculate the total anticholinergic burden. For men over 60, request a baseline bladder scan to ensure there is no significant residual urine before continuing the therapy.
If you're starting a new prescription, consider a "monitoring phase." This means scheduling follow-up appointments in the first month to check for changes in urinary flow. If you notice any of the danger signs-like straining or a weak stream-contact your provider immediately to discuss a dose reduction or a switch to a safer alternative like a beta-3 agonist.


Sam Hayes
April 4, 2026been through this with my old man and it is no joke. the bladder scan is the only way to be sure before starting meds so definitely push for that if you are in this boat
Mark Zhang
April 5, 2026It's really helpful to have the specific numbers like the PVR threshold mentioned here. For anyone feeling overwhelmed, just take it one step at a time and keep a log of your symptoms to show your doctor. You've got this!
Vicki Marinker
April 5, 2026The premise is fundamentally simplistic. One fails to consider the psychological toll of chronic urinary issues, which often outweighs the pharmacological risks discussed in this sterile summary.
Lawrence Rimmer
April 6, 2026Typical medical reductionism. We treat the bladder like a plumbing fixture rather than part of a complex biological system. It's all just switches and valves until you're the one staring at an ER ceiling.
Aysha Hind
April 6, 2026Oh please, this is just a tiny glimpse into the pharmaceutical rabbit hole! They push these 'selective' drugs because the patents are fresh and the money is flowing, not because they actually care about your prostate. It's a total shakedown by Big Pharma to keep us dependent on a cycle of meds and catheters. Absolute madness if you actually think the 'guidelines' are for our benefit. Just follow the money trail and you'll see why these risks are downplayed until you're literally bursting at the seams. It's a rigged game, folks, a total circus of medical greed and calculated negligence!
simran kaur
April 8, 2026The data provided is suspiciously convenient. I find it quaint that people believe these percentages are gathered without an agenda. It's quite obvious that the narrative is steered to favor newer, more expensive agonists.
Hudson Nascimento Santos
April 9, 2026There is a certain irony in the struggle between the desire for control and the loss of basic bodily function. We seek to master our biology with chemistry, only to find ourselves enslaved by the side effects of that very mastery.
sophia alex
April 10, 2026Imagine thinking a little pill is the solution to everything 🙄 Only in America do we think we can just medicate away the aging process. This is just pathetic! 💅
Dee McDonald
April 11, 2026STOP waiting for things to happen! If you're over 60 and on these drugs, get your bladder scanned NOW! Don't let a lazy doctor just shrug off your symptoms. Be your own advocate or you'll end up in the ER!
Jenna Carpenter
April 11, 2026honestly some of u guys just dont get how dangerus this is. like my uncle tried this stuff and it was a total disaster. read the warnings ppl!!
Brian Shiroma
April 13, 2026Sure, because nothing says 'healthcare' like waiting until you can't pee for 12 hours before realizing the meds aren't working. Truly a masterclass in preventative medicine.
Rachelle Z
April 14, 2026Wow... just wow!!! 🙄 Who knew that blocking the 'on switch' for peeing might actually... stop you from peeing??? 🤯 Absolute genius logic there!!! 🌈✨
Dipankar Das
April 15, 2026I must insist that all patients approach this with utmost diligence! It is imperative that you strictly adhere to the monitoring phases described here to ensure your wellbeing is never compromised!
Hope Azzaratta-Rubyhawk
April 17, 2026Everyone must take a stand for their health! Do not settle for subpar care or outdated prescriptions when safer alternatives exist. Demand the beta-3 agonists and take charge of your life immediately!